
The impact of fixed-dose anatihypertensive therapy on cardiorenal syndrome markers in patients with acute coronary syndrome and comorbidities
Authors
-
Sergey A. Pribylov
Belgorod Regional Clinical Hospital of St. Joasaph, Belgorod, Russia
 https://orcid.org/0000-0002-2913-493X
https://orcid.org/0000-0002-2913-493X
-
Kristina O. Leonidova
Kursk State Medical University, Kursk, Russia
https://orcid.org/0000-0001-6120-6748
-
Vladislav S. Pribylov
Kursk Regional Multidisciplinary Clinical Hospital, Kursk, Russia
https://orcid.org/0000-0002-4545-9339
-
Evgeniya V. Gavrilyuk
Kursk State Medical University, Kursk, Russia
https://orcid.org/0000-0001-5904-2828
-
Nadezhda N. Pribylova
https://orcid.org/0000-0001-6788-518X
-
Lvovskaya A. Mikhailovna
Kursk State Medical University, Kursk, Russia
https://orcid.org/0009-0004-8916-7073
DOI:
https://doi.org/10.18413/rrpharmacology.12.1055Abstract
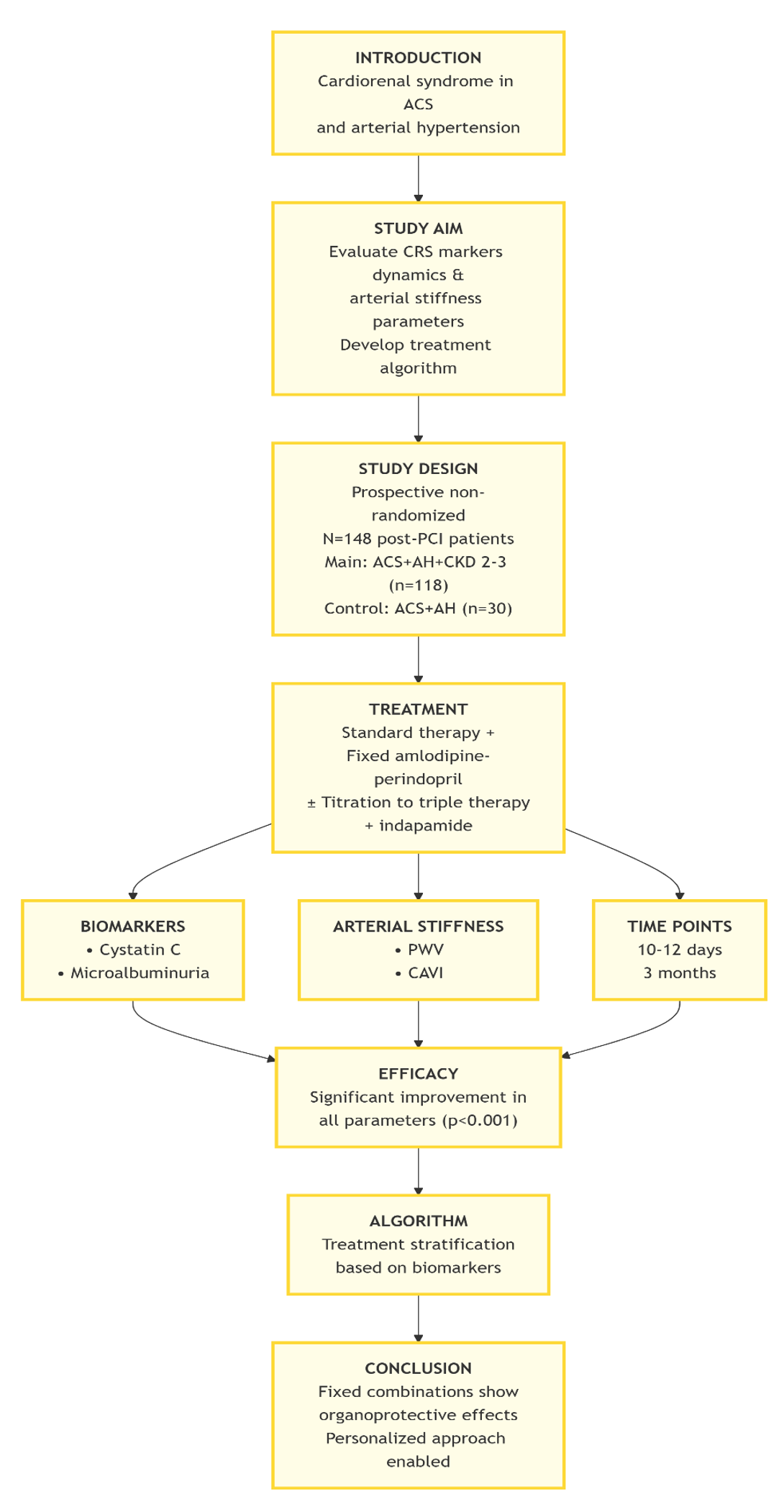
Introduction: The problem of cardiorenal syndrome (CRS) in patients with acute coronary syndrome (ACS) and arterial hypertension (AH) is highly relevant. Early diagnosis, based on cystatin C, microalbuminuria, and arterial stiffness, is key for prognosis and therapy selection. Aim: To assess CRS marker dynamics and arterial stiffness in patients with ACS, AH, and chronic kidney disease (CKD) on standardized therapy, and to develop a treatment selection algorithm.
Materials and Methods: A prospective study included 148 patients after percutaneous coronary intervention for ACS with AH. The main group (n=118) had CKD stages 2-3; controls (n=30) had no CKD. All received initial therapy with a fixed-dose combination of amlodipine 5 mg/perindopril 5 mg once daily, with possible uptitration to a triple combination including indapamide 1.25 mg (amlodipine 5 mg/perindopril 5 mg/indapamide 1.25 mg once daily). Markers were assessed at days 10-12 and 3 months.
Results: Cystatin C and microalbuminuria correlated with ACS severity and arterial stiffness. After 3 months, the main group showed significant improvement: cystatin C decreased from 1.35±0.33 to 1.02±0.29 mg/L; microalbuminuria – from 41.24±3.56 to 25.56±2.99 mg/L; pulse wave velocity – from 9.31 to 8.20 m/s (all p<0.001). Triple therapy provided a more pronounced effect. Baseline cystatin C >1.3 mg/L and microalbuminuria >30 mg/L are criteria for considering early triple therapy initiation.
Conclusion: Standardized therapy with perindopril/amlodipine, with the possible addition of indapamide, significantly improves cardiorenal status and vascular stiffness. The developed algorithm, based on initial biomarkers, allows for a personalized approach to managing these comorbid patients.
Graphical Abstract
Keywords:
cardiorenal syndrome, acute coronary syndrome, chronic kidney disease, cystatin C, microalbuminuria, arterial stiffness, Amlodipine, perindopril, indapamide, fixed-dose combinations, treatment algorithm, personalized medicineReferences
Barzilay JI, Farag YMK, Durthaler J (2024) Albuminuria: An underappreciated risk factor for cardiovascular disease. Journal of the American Heart Association 13(2): e030131. https://doi.org/10.1161/JAHA.123.030131 [PubMed] [PMC]
Chen DC, Potok OA, Rifkin D, Estrella MM (2022) Advantages, limitations, and clinical considerations in using cystatin C to estimate GFR. Kidney360 3(10): 1807–1814. https://doi.org/10.34067/KID.0003202022 [PubMed] [PMC]
Jankowski J, Floege J, Fliser D, Bohm M, Marx N (2021) Cardiovascular disease in chronic kidney disease: Pathophysiological insights and therapeutic options. Circulation 143(11): 1157–1172. https://doi.org/10.1161/CIRCULATIONAHA.120.050686 [PubMed] [PMC]
Lage JGB, Bortolotto AL, Scanavacca MI, Bortolotto LA, Darrieux FCC (2022) Arterial stiffness and atrial fibrillation: A review. Clinics (Sao Paulo) 77: 100014. https://doi.org/10.1016/j.clinsp.2022.100014 [PubMed] [PMC]
Lees JS, Fabian J, Shlipak MG (2024) Cystatin C should be routinely available for estimating kidney function. Current Opinion in Nephrology and Hypertension 33(3): 337–343. https://doi.org/10.1097/MNH.0000000000000980 [PubMed]
Pribylov SA, Leonidova KO, Pribylov VS, Gavrilyuk EV, Pribylova NN (2024) Approaches to therapy Amlodipine/Indapamide/Perindopril therapy of high arterial hypertension in ischemic heart disease patients with chronic kidney disease stage 1-3 after coronary stenting. Research Results in Pharmacology 10(2): 49–55. https://doi.org/10.18413/rrpharmacology.10.475
Pribylov SA, Yakovleva MV, Pribylov VS, Barbashina TA, Leonidova KO, Pribylova NN (2022) Arterial rigidity in patients with acute coronary syndrome without persistent ST-segment elevation in combination with chronic kidney disease and arterial hypertension and its correction against the background of antihypertensive therapy. Man and His Health [Chelovek i Ego Zdorov’e] (1): 19–27. https://doi.org/10.21626/vestnik/2022-1/03 [in Russian]
Virani SS, Newby LK, Arnold SV, Bittner V, Brewer LC, Demeter SH, Dixon DL, Fearon WF, Hess B, Johnson HM, Kazi DS, Kolte D, Kumbhani DJ, LoFaso J, Mahtta D, Mark DB, Minissian M, Navar AM, Patel Z, Piano MR, Rodriguez C, Stevens AW, Virani SS, Williams KA (2023) 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the management of patients ith Chronic coronary disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 148(9): e9–e119. https://doi.org/10.1161/CIR.0000000000001168 [PubMed]
Xu S, Ilyas I, Little PJ, Li H, Kamato D, Zheng X, Luo S, Li X, Weng J (2021) Endothelial dysfunction in atherosclerotic cardiovascular diseases and beyond. Pharmacological Reviews 73(3): 924–967. https://doi.org/10.1124/pharmrev.120.000096 [PubMed]
Zhivtsova NYu, Brezhneva EM, Lysenko AA (2024) Problems of diagnosis and treatment of acute coronary syndrome in patients with chronic kidney disease. Complex Problems of Cardiovascular Diseases [Kompleksnye Problemy Serdechno-Sosudistykh Zabolevanii] 13(3S): 120–135. https://doi.org/10.17802/2306-1278-2024-13-3S-120-135 [in Russian]
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Pribylov SA, Leonidova KO, Pribylov VS, Gavrilyuk EV, Pribylova NN, Lvovskaya AM

This work is licensed under a Creative Commons Attribution 4.0 International License.
 Русский
Русский
 English
English

